
The Hard Limit on Human Lifespan
Why Motor Neurons Are the Final Boss of Longevity


The manor has stood for nine decades. Its wiring was laid down in the first months of construction—electrical sockets embedded in the walls that would never be replaced, because the blueprints were lost long ago and no contractor knows how to add new ones.
For most of its life, the lights worked fine. But now, late in the manor’s life, sockets are failing faster than ever. The lights are going dim. And no one has the repairman’s number.
This is the story of human aging.
Human lifespan is not primarily limited by cancer, cardiovascular disease, or metabolism. It is limited by the irreversible loss of motor neurons—the wiring required to move, breathe, and cough.
The Problem the Calculator Revealed
When I first built the True Age calculator, the math kept producing impossible results.
Every longevity intervention—walking, exercise, diet—reduces all-cause mortality by some percentage. Stack enough together and the calculator should show extended lifespans. It did. The problem was it kept showing them past age 100—lifespans of 125, 130, or more.
The fix was simple but revealing: I had to zero out intervention effects around age 100. The interventions that powerfully reduce mortality at 60 or 70 stop working at extreme ages. Something else takes over—something the interventions don’t touch.
If baseline all-cause mortality hazard is multiplied by intervention effects (HR₁ × HR₂ × HR₃ …), the model predicts survival beyond 120. Empirically, this never happens. Longevity YouTubers Tony Ruggia and Dr. Michael Lustgarten have highlighted the missing variable as a non-modifiable age-dependent hazard driven by neuromuscular failure.
That something is motor neuron loss.
My father’s biomarkers are excellent. His mind is sharp. At 90, he has difficulty walking across a room. This is what motor neuron decline looks like from the outside—and no amount of optimized bloodwork changes it.
The Wiring You’re Born With
Motor neurons are among the most irreplaceable cells in the human body. Their axons stretch up to one meter from the spinal cord to muscles in the feet—some of the longest cells in the body. While the brain contains 86 billion neurons, your ability to move every voluntary muscle depends on just 150,000 motor neurons1.
These neurons appear by the fourth week after conception. Neurogenesis is complete by mid-second trimester. After that, no new motor neurons are ever made. The ones you have at birth are the ones you’ll have for life.
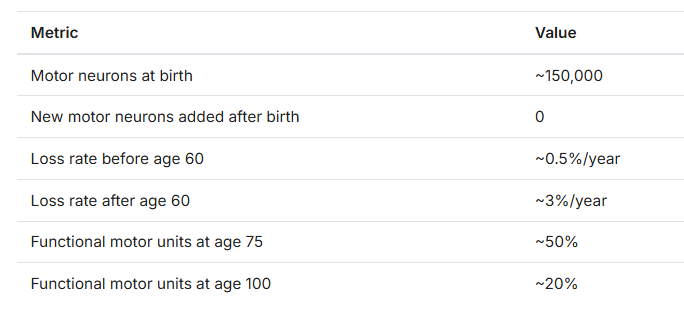
The Motor Neuron Ceiling: Based on observed motor unit loss rates (~3%/year after 60), functional collapse occurs when motor unit availability falls below ~20-25%. In humans, this threshold is consistently reached between ages 110-120, regardless of metabolic health or disease avoidance.
The Manor
The motor neuron system maps onto our aging manor.
The electrical sockets are motor neurons—fixed at birth, never replaced, slowly failing over decades.
The wires running to each lamp are neuromuscular junctions (NMJs), the connections between neurons and muscle fibers. Recent research shows these degrade first—the wires fray before the sockets burn out2.
The lamps are muscle fibers. They do the actual work of movement.
The repairman who could add new sockets? He doesn’t exist. No one has his number. The manor must make do with what it has.
Nobody Escapes This
There are two ways to die: from a disease, or from frailty.
Beat cancer. Survive cardiovascular disease. Avoid diabetes, infections, accidents. Live long enough, and neuromuscular failure gets you anyway. There is no third option.
A population-based study of over 35,000 English centenarian deaths shows the shift3:
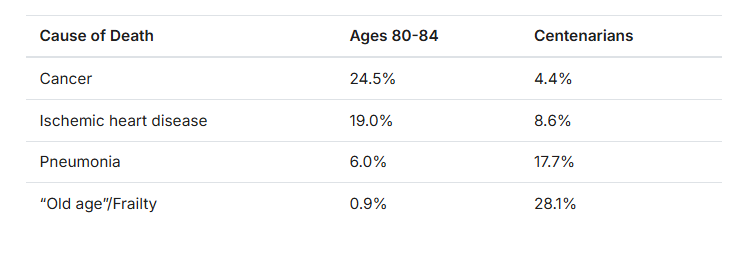
At ages 80-84, less than 1% of death certificates list “old age” as the primary cause. By 100, it’s 28%—and if you include both primary and contributing causes, 76% list “old age.”
Cancer and heart disease become almost irrelevant. Centenarians have outlived those diseases. What they cannot outrun is the progressive failure of the neuromuscular system.
The pneumonia spike reveals the mechanism. Frailty doesn’t just increase vulnerability to pneumonia—it makes pneumonia unsurvivable. Coughing requires explosive activation of the intercostals and abdominals, generating intrathoracic pressures of 200+ mmHg4. When motor unit loss crosses a critical threshold, the body can no longer generate the force to expel fluid from the lungs. The infection a 70-year-old would cough away becomes fatal at 100 because the neuromuscular machinery for coughing no longer works.
Maria Branyas Morera: Case Study in Optimal Aging
Maria Branyas Morera died in 2024 at age 117 years and 168 days. She represented the ceiling of what current longevity knowledge can achieve.
By the three-system framework I use to evaluate longevity interventions: her metabolic health was exceptional—a 2025 analysis of her blood, gut bacteria, and cellular markers found her mitochondria aged more slowly than average. Her inflammation markers were low, with a gut microbiome rich in inflammation-fighting bacteria. Her cardiovascular system was sound, with exceptional cholesterol levels and rare genetic variants for disease resistance. Researchers concluded that “extremely advanced age and poor health are not intrinsically linked5.”
Her cognition remained sharp. She played piano until 108. She survived COVID-19 at 113.
Yet she had been in a nursing home since age 93—over two decades—because her mobility had deteriorated to the point where independent living was impossible.
She died “peacefully in her sleep.” Tony Ruggia speculated the most likely mechanism is respiratory muscle failure—the diaphragm lacked sufficient neuromuscular function to continue breathing6. No disease. No infection. Just the final failure of the wiring that moves the muscle that moves the air.
The vascular system was fine. The immune system was fine. The metabolic system was fine. None of it mattered.
Her lifespan was not limited by inflammation, cardiovascular disease, cognition, or infection—but by respiratory motor unit loss, exactly as the model predicts.
The Sprouting Trap
The chart below shows motor unit number estimation (MUNE, orange)7 and grip strength (blue)8 plotted against age. Both are normalized to peak values, with the red zone indicating the mobility impairment threshold at 40% of peak grip strength.

Notice how the two lines track together until around age 60-70, then diverge—strength falling faster than motor units. This is the sprouting trap in action.
When sockets start failing, the manor has a clever workaround. Surviving sockets can extend new wires to take over the lamps that lost their connection. One socket that used to power one lamp can now power two, then three. For decades, this keeps the lights on.
Motor neurons do exactly this. A 1978 study by Brown and Ironton showed that motor neurons could sprout to innervate up to five times their normal territory after partial denervation9. This compensation works remarkably well at first. Surviving motor units expand their territory, rescuing denervated fibers and preserving muscle mass. Strength remains relatively stable through the seventh decade despite significant motor unit loss.
But this is borrowing against the future.
Each sprouting event loads more muscle fibers onto a single motor neuron. The enlarged units experience increased oxidative stress. Their NMJs become less stable. The signal that once precisely controlled 100 muscle fibers now tries to orchestrate 500.
When most sockets have already failed, the few survivors are each running at maximum capacity—five lamps per socket instead of one. The wiring is overloaded. And when you try to plug in that sixth lamp, the whole circuit blows. All five lights go dark at once.
Gordon, Hegedus, and Tam documented this transition from adaptive to maladaptive sprouting in 200410. Around age 75-80, the tradeoff comes due. When fiber-to-neuron ratios exceed that 5x threshold, sprouting stops being compensation and becomes the cause of failure. The overloaded neurons start failing. When one finally dies, it doesn’t just take its original muscle fibers—it takes all the orphaned fibers it adopted over decades. The mechanism that delayed muscle loss now accelerates it.
Sprouting progression:
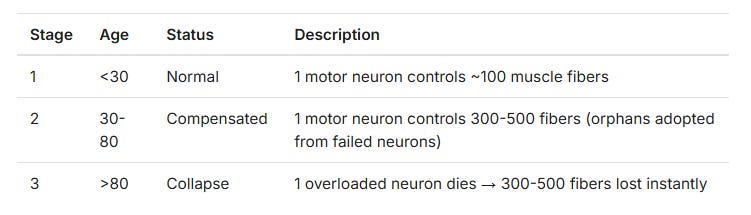
Strength falls slowly at first, then all at once. Look at the chart again—after age 75, the strength line collapses toward the red zone while motor units continue their steady decline. Grip strength below ~40% of young adult norms corresponds to loss of independent ambulation, inability to rise from a chair without assistance, and sharply increased pneumonia fatality—making it a practical frailty threshold rather than a statistical artifact.
The Strength-Motor Unit Disconnect
This divergence has a name: dynapenia—loss of strength independent of muscle mass.
You may have heard of sarcopenia—the loss of muscle mass with age. Sarcopenia is relatively tractable: strength training builds muscle, protein supports it, and even older adults can gain mass with proper stimulus.
Dynapenia is different. It’s the loss of strength even when muscle mass is preserved. It occurs because the surviving motor units can’t function at capacity—overwhelmed by too many adopted muscle fibers, unable to coordinate signals across expanded territory, running through unstable NMJs. Those over 75 activate significantly larger motor units per newton of force11. The system works harder to produce less output.
For sarcopenia, we have a solution: train strength. For dynapenia? No solution in sight. The wiring is failing.
Why Strength Training Can’t Stop This
Strength training builds bigger, stronger muscle fibers. In our manor, this is like replacing 60-watt bulbs with 100-watt bulbs. The surviving sockets shine more brilliantly than before. This helps—when sockets are working. But when a socket fails, it doesn’t matter how bright the bulb was. The light goes out.
The second chart shows what happens when someone goes from untrained to trained. Resistance training in older adults yields approximately 22% gains in leg strength and 8% gains in grip strength12. That 22% leg strength boost sounds significant. But grip strength—the metric most predictive of mortality—improves by only 8%.

Look at what that 8% advantage actually buys. The untrained person crosses the 40% grip strength threshold—mobility impairment—at around age 97. The trained person crosses it at 99. Two years. Decades of training translate to an additional two years before mobility impairment.
The Centenarian Evidence
The Georgia Centenarian Study measured grip strength in 244 centenarians. Average: 12.7 kg for men—about 25% of young adult strength13.
Edith Murway-Traina, the world’s oldest competitive powerlifter, could deadlift 68 kg at age 10014. That’s roughly what an untrained 30-year-old woman could lift on her first day in the gym. A lifetime of strength training, and she was back to beginner level.
Long-term athletic training does not prevent age-related loss of motor units. Master athletes show similar motor unit losses to sedentary controls of the same age15. Elite lifters don’t escape frailty significantly longer than sedentary people. When motor unit numbers drop below 20%, even doubled strength collapses below the functional threshold.
Strength training at 50 means better quality of life at 70. It means more functional capacity during the decades when the interventions actually work. Strength training meaningfully improves area under the curve of function, not the endpoint. It does not delay the final collapse.
The Research Landscape
The longevity field loves its frameworks. Twelve hallmarks of aging. Seven types of cellular damage. Eleven pathways to target. Researchers chase telomeres, autophagy, NAD+, senolytics. Supplement enthusiasts stack resveratrol, spermidine, and quercetin.
None of it touches motor neuron decline.
The molecular pathways governing NMJ maintenance are known. Researchers have demonstrated that manipulating these pathways can affect NMJ function in animal models. But when you look at what interventions actually get tested, it’s the same recycled list: caloric restriction, resveratrol, exercise16.
Caloric restriction doesn’t prevent motor neuron loss in humans. Resveratrol has failed in human trials for essentially everything. Exercise helps muscle quality but doesn’t prevent age-related motor unit loss—master athletes lose motor units at the same rate as sedentary controls17. The pathways are known. The therapeutic development isn’t happening.
What Would Actually Help
If humanity wants to break past the current lifespan ceiling, we need therapies that:
Slow sprouting before the collapse — Reduce the rate at which surviving neurons adopt orphaned fibers, delaying overload
Prevent NMJ degradation — Stabilize the connections before they fragment
Restore degraded NMJs — Rebuild the wiring after damage occurs
The molecular targets exist. The Agrin/MuSK/Lrp4 signaling pathway governs NMJ formation and maintenance—agrin released from nerve terminals activates MuSK receptors to cluster acetylcholine receptors at the junction. Neurotrophic factors like GDNF (glial cell line-derived neurotrophic factor) support motor neuron survival. These aren’t speculative—they’re identified pathways with demonstrated effects in animal models, and ALS research has validated them from both directions: block MuSK and junctions fail; enhance GDNF and motor neurons survive longer18.
What’s missing is someone to actually turn this biology into treatments—whether that’s drugs targeting NMJ stability, microsurgical techniques to restore connections, or epigenetic interventions to reset junction function.
Consider what happened with obesity. For decades, the advice was “eat less, move more”—and it barely worked. Then GLP-1 receptor agonists came along. Drugs like semaglutide (sold as Ozempic and Wegovy) transformed the field almost overnight. Obesity went from an intractable willpower problem to a treatable medical condition.
Motor neuron maintenance is waiting for its GLP-1 moment. The biology is tractable. The targets are identified. Even a perfect NMJ-stabilizing therapy would not create immortality—but it could plausibly extend the functional lifespan ceiling from ~120 toward ~135 by slowing late-life motor unit collapse. Someone just needs to pursue it seriously.
The Key to 130
Most of my posts end with something you can do: eat this, walk that, train this way.
This post is different. Strength training helps—do it for quality of life in your 60s and 70s. But understand what it can and cannot achieve. It builds stronger muscle fibers. It does not repair the wiring. It does not prevent motor neuron loss.
My father has excellent biomarkers. His mind is sharp. At 91, he struggles to cross a room. Maria Branyas had perfect biomarkers. She spent 24 years in a nursing home. No one escapes this—yet.
Remember the manor’s missing repairman? The one who could add new sockets or fix broken wiring? He exists somewhere. The molecular pathways are identified. The biology is tractable. Someone just needs to find him.
The 120th and 130th decade of human life are locked behind a door, and the key is motor neuron maintenance. The longevity field needs its GLP-1 moment for frailty—someone to actually develop these pathways into therapies. The biology is waiting.
Find the repairman.
I found this really intriguing. You raised some excellent points here, Crissman.